Hi experts,
I’m trying to segment the GM and WM using T2s (generic protocol) on about 20 patients.
The patients I am scanning have GM/WM pathology and atrophy, and I’ve noticed deepseg_gm doesn’t work perfectly (especially around the borders of the GM, where the configuration of the GM seems to be very unusual in this cohort!)
Any tips for segmenting using e.g., propseg? Or any parameter choices that may assist before I go down the manual seg route? See attached.
Thanks!
-Thomas Shaw
sub-015_ses-01_run-1_T2starw.nii.gz (4.3 MB)
The patients I am scanning have GM/WM pathology and atrophy, and I’ve noticed deepseg_gm doesn’t work perfectly (especially around the borders of the GM, where the configuration of the GM seems to be very unusual in this cohort!)
There is indeed obvious hyperintense signal around the lateral corticospinal tract. I’m not exactly sure what you mean by “deepseg_gm doesn’t work perfectly”. Do you expect the algorithm to segment the entirety of the hyperintense signal? Personally I would not, since part of the hyperintense signal is in the WM (not the GM). I’m curious what you would expect from the segmentation-- maybe you can show us how you would do it manually, so we have a better sense? Regardless, I find it extremely difficult and unreliable to segment the GM on these images (whether manually or automatically), because we cannot confidently identify the boundaries of the GM. I would instead rely on a probabilistic mapping of a GM template via registration to the PAM50.
Hi Julien,
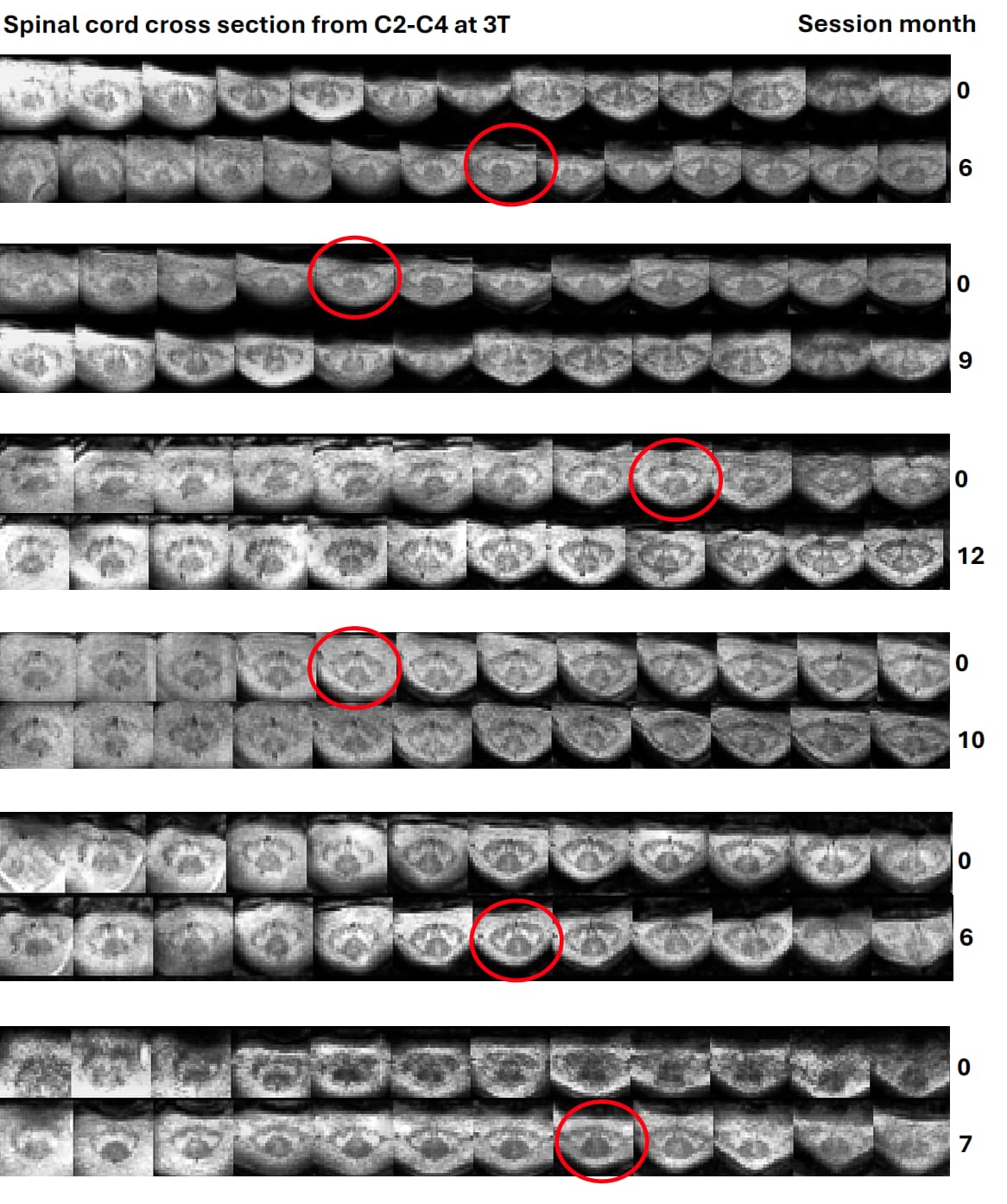
This hyperintensity seems to be consistent for each of the participants (see below for 6 patients scanned at two timepoints, each)
To me, the GM configuration is consistently in a different shape (i have been calling it an “hourglass” shape) for each participant in this cohort.
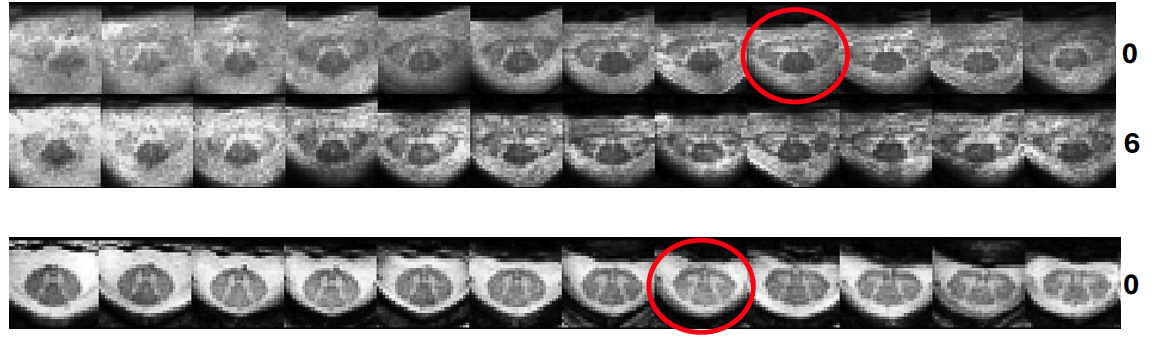
When I compare it to my control data:
You mentioned this may be a WM hyperintensity, rather than GM changes? This would be very interesting as well.
To answer your question: I would likely segment the hyperintense signal as GM. But I’m worried it would be unreliable as well.
There is a similar finding in *Frebourg et al., (2021), The good, the bad and the ugly : a retrospective study of image quality in human cervical spinal cord MRI at 7T. Proc. ISMRM 2021 https://www.ismrm.org/21/program-files/TeaserSlides/TeasersSessions/85.html (figure 5(g)), who describe it as “strong degeneration of lateral funiculi”
Thanks!
Hi Thomas,
Yes, WM hyperintensity in the CST of ALS patient has also been reported in another study (7-T MRI of the spinal cord can detect lateral corticospinal tract abnormality in amyotrophic lateral sclerosis - PubMed). So as I said earlier, i don’t think these hyperintensities belong to the GM, but rather to the WM. So including them in the GM mask would be wrong, in my opinion.
Cheers,
Julien